online assessment
Find out which treatment is right for you.
fix my smileFor further information about how we use your data, please see our privacy policy
By Daljit Gill BDS, BSc, MSc, FDS RCS, M.Orth, F.Orth RCS (Eng) Consultant Orthodontist, UCLH Eastman Dental Hospital, London UK.
All patient embarking upon orthodontic treatment should be aware of the possible adverse effects of treatment. Several of these effects are outlined below. It must be stressed that the vast majority of orthodontic treatment undertaken is NOT associated with significant adverse effects.
The mouth is populated by millions of bacteria that adhere onto both the tooth and mucosal surfaces. Some of these bacteria which populate the teeth produce acids from sugars that are ingested in the diet. If the frequency of sugar intake is excessive then too much acid is produced which results in tooth decay (also termed caries or decalcification).
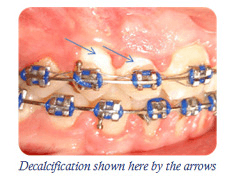
Whenever a fixed appliance is fitted onto the teeth, tooth cleaning becomes more difficult and the number of bacteria populating the mouth multiply. It therefore follows that the risk of dental decay around the orthodontic attachments will also multiply if the teeth are not kept meticulously clean. Orthodontic decalcification can produce decay marks on the front surfaces of teeth which can reduce the aesthetic success of orthodontic treatment. During treatment, your orthodontist will monitor your tooth brushing and advise you if it needs to be improved to prevent this complication from occurring. It is also necessary to follow the following advice:
Orthodontic appliances work by placing a gentle continuous force onto the roots of the teeth. A compressive force is always generated on the root surface in the direction of tooth movement. This compressive force also temporarily reduces the blood supply in the immediate area by squeezing the small blood vessels alongside the root surface. Through complex mechanisms, this will result in some of the root surface dissolving away temporarily. Not all the root surface is repaired following this which results in a permanent slight (1–2mm) shortening of the root. In only a very small number of patients.
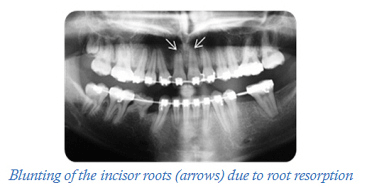
Your orthodontist can predict, with considerable success, patients more likely to exhibit significant resorption by studying the pre–treatment radiographs (x–rays). This can help to warn patients who may be particularly prone to this complication. Radiographs can also be taken during treatment to monitor if the roots are becoming shorter. Certain habits such as nail biting, pen chewing and digit sucking can increase the chances of root resorption by placing additional compressive loads onto the teeth.
There is large individual variation in the intensity of pain experienced by patients during fixed appliance therapy. Most will experience some pain that is caused by a localised inflammatory reaction around the tooth socket. The pain is usually dull in character and is made worse by placing pressure onto the teeth. It usually starts within a few hours after appliance placement or adjustment, increases over the next 24 hours, and decreases to baseline levels within 5–7 days. It may show variation within the day with greatest intensity in the evening and night. Mild pain killers, such as Paracetamol or Ibuprofen, can be used to control the discomfort.
It is common for the gums to swell slightly during orthodontic treatment because of plaque accumulation. This swelling will often resolve 1–2 weeks after appliance removal.
There is a risk that patients with pre-existing recession are at risk of further recession during orthodontic tooth movement. This risk can be minimised by ensuring that the teeth are kept clean, a non-traumatic brushing technique is used and that regular visits to the hygienist are scheduled during treatment. Your orthodontist will also closely monitor the recession during treatment to ensure that it is not progressing.
The top picture shows before treatment and the lower picture shows after treatment with progression of recession (arrows)
There is no evidence that orthodontic treatment can create problems with the jaw joints or make pre-existing jaw joint problems worse. Equally there is no scientific evidence that orthodontic treatment can treat jaw joint problems in the majority of individuals.
